By Jacqline Wolf Tice, B.S. CHES
Cumulative national data on breastfeeding is cause for some optimism, according to the CDC’s 2014 Breastfeeding Report Card. The national trends in exclusive breastfeeding (EBF) at 3- and 6-months have each increased 2-3 percentage points from previous year rates (as reported in the 2013 Breastfeeding Report Card). The report states that nearly 41% of children born in the U.S. are being exclusively breastfed at 3-months, and the rate for babies exclusively breastfeeding at 6-months, is 18.8%. That's nearly 1/5 of all U.S.-born babies! With only five years to go, we may actually reach the Healthy People 2020 objectives of 46.2% of babies EBF at 3-months and 25.5% EBF at 6-months.
The overall increase in these numbers is due, in part, to three components:
The number of babies NOT given formula in the first two days of life. (Babies who are breastfed in the first two days of life are more likely to be breastfed after leaving the birth facility.)
The number of IBCLC's and CLC's per 1,000 births. (Evidence-based maternal education and support mechanisms regarding breastfeeding increases likelihood of breastfeeding.)
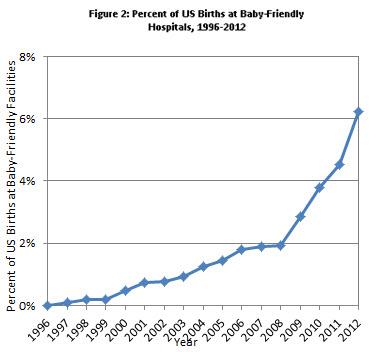
The impact of the Baby Friendly Hospital Initiative in the U.S. (Implementation of The 10 Steps into hospital policy has created a supportive environment that generates expectation for babies to be fed breast milk.)
Institutional policies supportive of breastfeeding are essential and are driving factors that promote normalization of EBF as the first option in infant feeding. As well, implementation of the Patient Protection and Affordable Care Act, with its policy directive mandating businesses (with 50+ employees) to accommodate breastfeeding mothers, has also helped lay the groundwork for increasing EBF rates.
In the efforts to achieve greater breastfeeding rates, however, there is a deeper and more far-reaching component, common to countries like Norway and Sweden, that has remained elusive in the U.S. That is the awareness of the social contract component inherent in breastfeeding. With medical, public health, and government experts in agreement that breastmilk is the most healthy and economical feeding option for nearly every infant until 6 months of age, it should follow that EBF be considered morally right and normal (and expected). Acceptance and support for mothers and families who choose EBF ought to generate compassion and admiration, not embarrassment and shame, when encountered in the public sphere. That is a central tenet of social contract theory - normalization of social practices supported by public policies based on assumptions all would (or do) agree are beneficial for all.
While it is easier to access long-range data and support about the health and psycho-emotional benefits of breastfeeding for both babies and mothers, breastfeeding is generally still stigmatized in social environments in the U.S. Community-based efforts and information delivery to mothers and their families from pre- through post-natal pregnancy is required to activate the "normalcy" demand for breastfeeding necessary to ensure each baby's right to be breastfed and each mother's right to breastfeed, wherever they are together.
The World Health Organization's Breastfeeding Policy Brief encourages community-based strategies including locally-tailored communication campaigns, peer-to-peer models, support groups, and engagement with community leaders to promote education and acceptance of EBF. In order to promote and activate normalcy of breastfeeding as part of a social contract, formally or informally, community champions are an essential and primary part of the equation.
Five years ago, we could not, as a society, have imagined there could be normalcy of prophylactic mastectomies to protect women against breast cancer. Yet, in women with BRCA1 or BRCA2 gene mutations, this surgery, championed by actor Angelina Jolie, has quickly become socially accepted, in part due to its 95% risk reduction of breast cancer in women with those specific gene mutations. The celebrity of Ms. Jolie became the driver of the information, triggering massive media attention, analysis, and social conversations which transformed how society interprets this issue.
But, do we really need celebrities to tell us how to interpret data? A 2002 meta-analysis published in Lancet looked at studies in 30 countries with over 150,000 women participants, with and without breast cancer, and found that breastfeeding could account for over two-thirds of breast cancer reduction incidence. Ovarian cancer risk is also reduced by breastfeeding. It is known that exclusively breastfed babies receive immunological protective factors for childhood conditions like diarrhea, lower respiratory infections, otitis media, necrotizing enterocolitis and pneumonia. There are also associations indicating decreased risk of asthma, Type 1 diabetes, and obesity in those who are breastfed. The benefits of breastmilk are well-documented and readily accessible. While celebrities do highlight the story, community champions help write the story.
It is difficult to change the way we think about our future and our children's futures when we are over-burdened with economic and personal issues that need our immediate attention. However, if human breast milk were bottled, sold in stores, and marketed like a popular energy drink, chances are it would fly off the shelves! In the U.S., we tend to value that which we must pay for. Breastmilk is free to every mother who gives birth and every baby she gives life to. Its value, though, as part of the social contract, is priceless.
Being a champion for breastfeeding means investing in this social contract and "paying it forward" through policy development, community engagement, and direct peer support - for the health and wellbeing of all our futures.
Jacqline Wolf Tice is a Public Health Professional and is employed by St. Luke's University Health Network as a Community Health Educator. In 2015, Jacqline was elected Board Co-Chair of the Lehigh Valley Breastfeeding Coalition.
Editor’s Notes:
Links to publications and data cited listed below were verified as of July 1, 2015.
Breast Cancer And Breastfeeding: Collaborative Reanalysis Of Individual Data From 47 Epidemiological Studies In 30 Countries, Including 50 302 Women With Breast Cancer And 96 973 Women Without The Disease*. The Lancet. July 2002. http://www.ncbi.nlm.nih.gov/pubmed/12133652?dopt=Abstract